
Shoulder Pain - What hurts and why?
Before discussing what can occur when things go wrong. We must first understand how the shoulder functions when things are going right. The shoulder joint proper – known as the glenohumeral joint, is made up of the shoulder blade (scapula) and the head of the arm (humerus). It is held in place similar to that of a golf ball (head of arm) on a tee (glenoid of scapula). To deepen the ‘socket’ (or tee) there is a structure known as a labrum that acts to create a larger surface and assist in stabilising the head of the arm in its socket. There are also many strong ligaments that reinforce this joint both at the front and back.
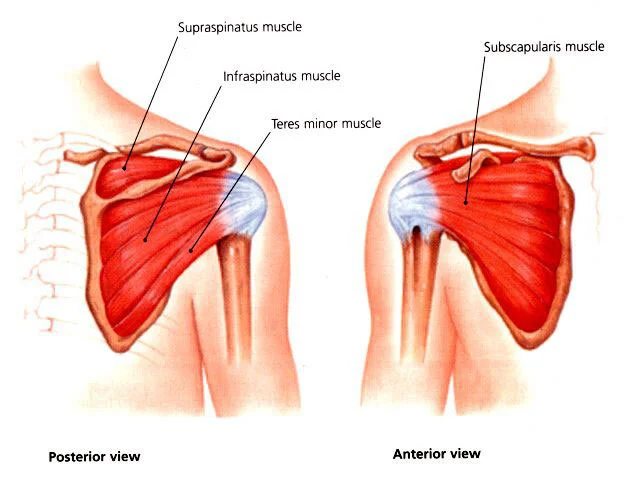
Another key structure of the shoulder is the rotator cuff muscle group. The rotator cuff assists with the movement of shoulder joint however due to the degree of movement they have a significant role in stabilising the shoulder joint. The rotator cuff by definition is comprised of 4 major muscles:
Subscapularis
Supraspinatus
Infraspinatus
Teres minor
These muscles act as a force-coupling unit to maintain the head of the arm in the centre of the ‘socket’ (glenoid) during movement of your arm and shoulder. Deficiencies in these muscles will affect how the arm moves within the shoulder and associated injuries may occur.
Shoulder pain is common among the population from young athletes to the elderly. The cause, structure duration and intensity of symptoms all very depending on a multitude of factors that may or may not include, age, demand of tasks/sport, duration of symptoms. The aim of this blog will be to shed some light on a few structures or problems that may arise in the shoulder and you can potentially do at home manage this pain in the short term.
Some common injuries/pathologies of the shoulder include, but are not limited to:
Rotator cuff injury
Labral tears
Shoulder dislocation
Shoulder fractures
Frozen shoulder

Rotator cuff pathologies make up approximately 80% of all shoulder complaints. However, this figure varies dependent on the age, occupation, sport/activity levels of an individual as the demand placed on the muscles varies with different tasks.
Rotator cuff tears are not common in young athletes but are typically seen as a consequence of degeneration or following an acute incident in older athlete/person. Tears can be classified as partial or full thickness in relation to the severity of the tear, and often present with pain in the front of the shoulder and difficulty when moving the arm overhead.
However, the presence of pain and difficulty moving the arm overhead may not always be indicative of a rotator cuff tear. Individuals/athletes who spend a lot of time with their arm overhead, or are performing tasks overhead including, tennis, throwing, painting etc are vulnerable to developing another extremely common rotator cuff injury. Rotator cuff tendinopathy may arise when there has been a change in load placed on a particular muscle (group) that is not conditioned to tolerate it, or when the tendon itself is experiencing compression. A tendinopathy is an irritation of the muscles’ tendon (the link between the muscle and bone) that can often become thicker than when it is not injured. Therefore, due to the increase in size, the tendon is at risk of compression, causing pain and consequently inhibiting function of the rotator cuff muscle group. This compression is often reported as impingement, notwithstanding that there are other examples of shoulder impingement, however these will be covered in a subsequent blog.
Like tendinopathies in other areas of the body, the most effective way to combat this injury is through correct loading principles and parameters, to activate the muscle and allow for the tendon to remodel and resemble its normal properties. Therefore, the primary approach to treating rotator cuff tendinopathy is through exercise. Depending on the irritability of your shoulder, how sensitive it is to movement, general advice surrounding lifestyle issues will also form a large portion of treatment, while focussing on selective exercises that will not exacerbate pain but load the cuff in a way to achieve the desired outcome – which is an overall improvement in function and reduction of pain. Recent studies have shown that people experiencing rotator cuff tendinopathies, that have accurately been assessed, diagnosed and managed can expect equivalent outcomes to surgical interventions in both short and long term follow up periods.
Diagnosis of shoulder pain or injury requires a thorough assessment with an understanding of the lifestyle factors that may be contributing to the cause of pain. If you are experiencing shoulder pain, and want to get to the bottom of it, Peter Stath Physio can help find the cause of the pain and work with you to develop a plan to get you back to your meaningful lie. Whether that be on the tennis court, in the swimming pool, or simply out in the garden, our physiotherapists will equip you with the strategies to empower you to take an active approach to your recovery to give you the best chance in obtaining an optimal outcome.
Keep an eye on the subsequent blogs of this series that will cover other injuries of the shoulder and how their presentations and management may potentially differ.
Pt 2 – Labral Tears
Pt 3 - Shoulder Dislocation
Pt 4 - Shoulder fractures
Pt – 5 Frozen Shoulder
References
Edmonds, E. W., & Dengerink, D. D. (2014). Common conditions in the overhead athlete. Am Fam Physician, 89(7), 537-541. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/24695599
Kinsella, S. B., & Carl, R. L. (2013). Upper Extremity Overuse Injuries. Clinical Pediatric Emergency Medicine, 14(4), 318-326.
Lewis, J. (2016). Rotator cuff related shoulder pain: Assessment, management and uncertainties. Manual Therapy 23, 57-68.
Lewis, J., McCreesh, K., Roy, J. and Ginn, K. (2015). Rotator Cuff Tendinopathy: Navigating the Diagnosis-Management Conundrum. Journal of Orthopaedic & Sports Physical Therapy, 45(11), pp.923-937.
Maloney, M., & Ryder, S. (2003). Diagnosis and management of rotator cuff tears. JOURNAL OF MUSCULOSKELETAL MEDICINE, 20(2), 87-92.
Murrell, G. A., & Walton, J. R. (2001). Diagnosis of rotator cuff tears. Lancet, 357(9258), 769-770. doi:10.1016/S0140-6736(00)04161-1
Pribicevic, M., & Pollard, H. (2004). Rotator cuff impingement. J Manipulative Physiol Ther, 27(9), 580-590. doi:10.1016/j.jmpt.2004.10.004